
Antibodies are studied more than other immune proteins for association with disease. This does not mean that they are more decisive in disease outcomes. Type I interferon likely has far more impact.
Antibodies Are Not the Whole Story of Immune Resilience Toward Cancer
Much is being made of a recent study showing IgG4 antibodies spiking in the blood labs of those who are triple-injected with the mRNA COVID vaccines. Journalists are speculating that this may be the cause of increased cancers in the COVID-vaccinated. But that is not the main reason that the COVID-vaccinated are getting new cancer cases, sometimes aggressive “turbo cancers,” or coming out of remission from earlier cancer. Rather, there is earlier research that provides more plausible mechanisms for cancer risk, based on abundant prior knowledge of immune function. Let’s look at both the new study on IgG antibodies and earlier research.
The popular fallacy seems to be along these lines: ‘Antibodies are easy to test for. Plus, they are the focus of vaccine development and vaccine action. So therefore we spend a lot of time thinking and talking about them. So therefore they must be important markers of disease outcomes. So therefore they must be decisive in disease outcomes.’
After focusing my own work on cancer patients for the last 16 years as a naturopathic oncologist, if I made this mistake in thinking, most of my patients would be dead by now from misdirected efforts.
No, cancer remains a mega-problem of DNA damage, immune distraction, disrupted cell signaling, frenzied growth, lack of apoptosis, weakened tissues, angiogenesis, and metabolic derangement, as the principal features of an entity that feeds itself at the expense and to the detriment of the organ and the organism. These are the principal features of cancer, and they are hard as heck to treat successfully. I discuss that very daunting challenge here.
IgG3 Versus IgG4
First, let’s look at the new study on IgG3 versus IgG4 antibodies in the triple-jabbed. Herein, let’s call it the IgG4 study. It finds that the triple-jabbed may be developing a non-inflammatory tolerance to even high levels of spike proteins. That is, rather than having typical dyspnea, cough, olfactory and other full-blown COVID-type symptoms, IgG4 is a tolerant and tolerizing antibody that allows virions and spike protein load to accumulate in the body without the usual symptomatic alarms. Thus, a COVID+ PCR result with mild symptoms, or even no symptoms, often ensues. This may partly account for the many celebrities and politicians frequently quoted in MSM saying in so many words, ‘I tested positive for COVID, but thanks to my shots, it’s mild.’ Yet their lack of effective immune defeat of SARS-CoV-2 is what prevents their developing a lasting neutralizing immunity. So they (at least at first) tolerate high spike protein loads and are perpetually vulnerable to recurrent infections. Even more worrisome, what underlies that recurrence of mild symptoms, show the IgG4 study authors, is a precarious derangement of immune function with potentially problematic stockpiling of viral load, spike proteins and antibodies, with potentially devastating consequences for their future health outcomes. Even a myeloma like abundance of immunoglobulins can create a multiple myeloma-like disease in the COVID-vaccinated, a sludgy protein-laden blood that is harmful to the fine filtration structures, glomeruli, of the kidneys.
That immune deviation, misdirection and derangement has been previously described as pathogenic priming, a maladaptation of the immune system to either ignore or to fight ineffectively against genuine threats, while at the same time focusing its resources to slay the paper tigers of non-threatening antigens. This happened in the design of the mRNA vaccines to produce a spike protein that was characteristic of the original Wuhan strain of SARS-CoV-2, but turned out to be ineffective against Delta, Omicron and subsequent strains, as some of us had earlier warned. Because the Wuhan strain had already flamed and burned out, the COVID vaccines were obsolete by the time they were offered to the public.
Under circumstances of natural infection, whereas IgM antibodies flare for a short time after infection onset, IgG antibodies, in contrast, are slower to develop, and are those that remain long after an infection has resolved. (For example, my measles IgGs are still robust on a blood lab decades after I had measles as a child, with only natural immunity, no vaccine history.)
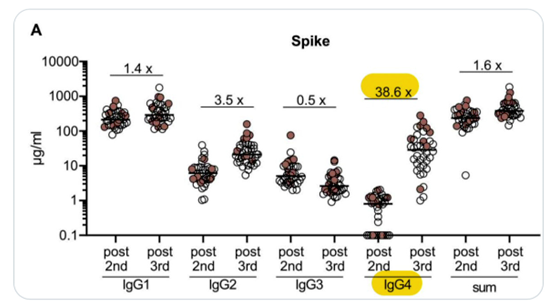
The subclass IgG4 is a non-inflammatory one that is correlated with tolerance to antigens, similar to allergy shots rendering the immune response more tolerant to grass pollen. IgG4 has no known effector function. Likewise, IgG4 seems to be inversely correlated with anaphylaxis. Here, in the IgG4 paper, regarding the COVID-vaccinated, IgG4 increases considerably, over 38 times, after a third mRNA injection. Please note that the scale of the y-axis is logarithmic, putting the IgG4s quite far up there.
At the same time, both triple- and double-jabbed lose a considerable amount of their IgG3 antibodies, discovered at 180-day and 210-day follow-up labs, respectively. Note again the logarithmic scale, showing cratering drop-off of IgG3 antibodies, with skyrocketing IgG4 antibodies. This is from Figure 1 of the IgG4 paper:
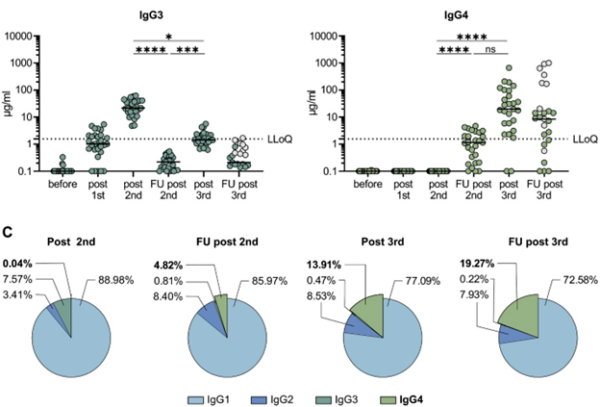
The subclass IgG3 is sometimes thought, including by the IgG4 authors, to be pro-inflammatory, one of many immune assaults against invading pathogens. Although there is evidence to the contrary as well. IgG3 is thus sometimes assumed, including by the IgG4 authors, and interested journalists, to neutralize, or fight effectively against, antigens.
However, there is little support, other than correlation of titers, for the assertion that IgG3 antibodies may be effective warriors against pathogens. The IgG4 study authors acknowledge an earlier observation of “IgG3 responses correlating with partial protection against HIV,” and only a rise in IgG3 antibodies after natural infection with SARS-CoV-2, such as reported here, without mechanism of its protection.
One possible clue as to the IgG4 study authors’ observations of low IgG3 is the glycosylation of IgG3 as impactful on SARS-CoV-2 infection severity. (Immunoglobulins are glycosylated protein molecules generally, but hyper-glycosylation seems to be a problem. Glycosylation is generally detrimental to its optimal function; notorious glycosylation has devastated more than simply antibodies, in our junk food loving culture.)
IgG3 antibodies are a very small proportion of IgG antibodies and have not yet been well-studied. Both IgG3 and IgG4 antibodies are generally a small proportion of all our B-cells, 3% and 4% respectively.
Low IgG3 antibodies are not necessarily correlated with low disease severity. For example, in COPD, we see this correlation of low IgG3 levels with life-threatening exacerbations of COPD. All antibodies, including IgG3 and IgG4, generally rise and then fall in case of natural infection. Below I will explain why I am not so sure the cause and effect vector goes as is currently being assumed, from low IgG3 / IgG4 ratio to generalized immune dysfunction. Rather, I suspect that it may more likely be an effect of other mechanisms, described below.
There Is so Much More to Immune Function Than Only Antibodies
The first problem with the current IgG fascination is the assumption that just because antibodies consume much attention, and are easily measurable proteins on a blood lab, that they are then necessarily impactful on the vast complexity of the rest of the immune system. Metaphorically, by assuming that that which we can see is necessarily decisive, we are looking at the skin, so to speak, and assuming that we therefore know the functions of the internal organs and that the skin is the dominant cause of internal effects. Obviously, such is not the case.
Let’s first assume that the highly mobile and ubiquitous blood contains many of the cells in our immune system and are, as a whole and in parts, key to optimal immune function. Here is the proportion of IgG immunoglobulin antibodies to the rest of the immune system:
Immunoglobulins are present on the surface of B-cells, where they act as receptors for antigens. B-cells fluctuate in number, but average 5.2% of all white blood cells. White blood cells are 0.1% of all cells in the blood. Therefore B-cells are about 0.00005% or 5 in 100,000 cells in the blood.
I explain further about that here.
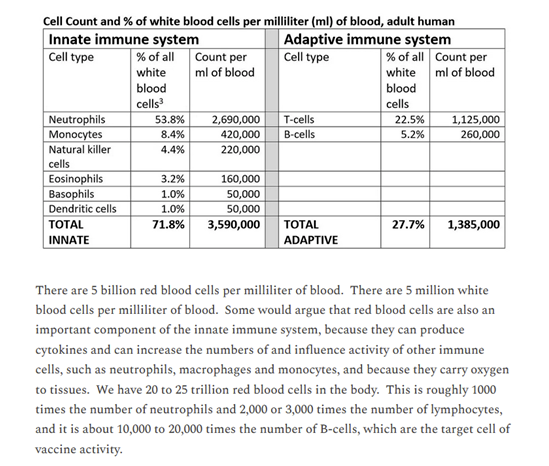
This proportion of B-cells to other cells in the blood is vanishingly small. If you can see the very skinny red line at the far left of the band below, that is the proportion of all B-cells compared to the vast remainder of cells in the blood. (The thin red line would actually need to be a little thinner to be true to scale.)

Now let’s look at other aspects of immune function that are powerhouse fighters against cancer, but have been associated with high viral load and/or high spike protein, such as is expected to occur after COVID vaccination. These researchers found that two of our most important cancer-fighting cells, natural killer (NK) cells and CD8+ T-cells were significantly reduced in these circumstances. Reduction in NK cells is seen with more aggressive tumors.
But the major problem with the mRNA COVID vaccines and cancer risk was shown in April of this year, in the Seneff, Nigh paper.
The science community’s pre-occupation with the relatively smaller adaptive immune system, mostly its humoral portion, and unfamiliarity or disinterest in the vastly more important and stronger innate immune system has led attention away from this seminal paper. I have to recommend not only reading but thoroughly studying the Seneff, Nigh paper for the best understanding to date of the effect of the COVID vaccines on tumorigenesis, immune-failure with respect to cancer and metastatic events.
What Seneff et al found is that the most profound threat to immune function by the mRNA vaccines is the interference with Type I interferon signaling pathways. This in turn debilitates the surveillance capabilities of the immune system in cancer detection. As a result, we see both new tumors and metastases of existing cancers in the COVID-vaccinated. We see what is now called turbo cancers. Here is how Seneff et al supports that hypothesis. Their paper is enormously detailed, and my summary of it below is quite brief.
Ivanova, et al found that people who were naturally infected with SARS-CoV-2 have been able to dramatically up-regulate our arguably most crucial cytokine, Type I interferon, as seen from their peripheral dendritic cells, whereas mRNA-vaccinated people have not shown this ability, nor any such increase, nor any progenitor cells for the same. From those various findings, is evident that the COVID vaccines suppress Type I interferon signaling. The results are a devastating breakdown of many downstream immune functions, creating new vulnerability to not only viral diseases, but also to cancer. The necessity of interferons for the body’s war against cancer is further seen in the productive clinical use over decades of interferon as a therapeutic agent to cancer patients.
The most appreciated mechanisms of Type I interferon against cancers include up-regulation of the tumor suppressor gene p53, as well as kinase inhibitors, and the resulting arrest of cancer’s cell reproduction. Perhaps even more crucial is that Interferon-alpha, a type of interferon I, makes cancer recognizable, or in a way visible to other immune cells for destruction. Two other major effects of Type I interferons, specifically interferon-alpha, are cell differentiation and apoptosis, which are two of the major events that are important for a natural victory over cancer. Type I interferon also activates the essential cancer-fighting cells discussed above, CD8+ and NK cells. There are further genetic effects of Type I interferons, each of which tend to suppress tumors, notably through IRF-7 genes. These genes have impact on cancers of the breast, prostate, uterus, ovaries and pancreas. But these and oncogenes generally appear to become dysregulated by the mRNA vaccines.
Fay et al discuss G-quadruplex formations in RNA, and that role in proto-oncogene expression. This can in turn lead to cancer progression.
Cancer Incidence
Even before the boosters were rolled out to the public, the Vaccine Adverse Events Reporting System (VAERS) of the Dept of Health and Human Services (HHS) showed vastly more cancers following COVID vaccines than for all other vaccines during the 30-year history of VAERS. These new cancers following the COVID vaccines accounted for 98% of cancers reported. Here again from Seneff et al:
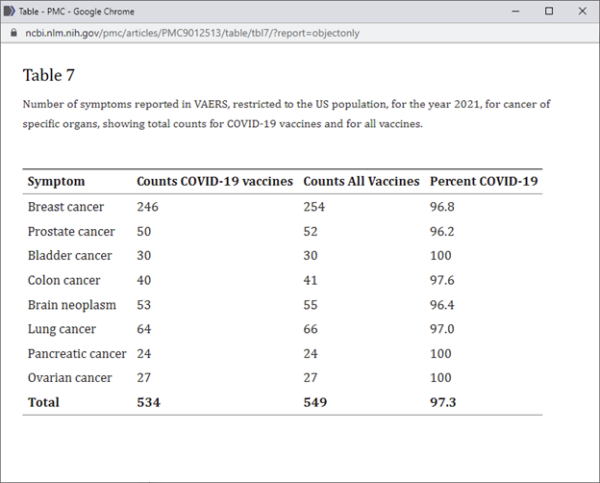
It should be noted that the reporting of these 2021 cancers occurred in large part prior to the US public’s (tepid) uptake of even the earliest mRNA COVID boosters (injection #3 in the fall of 2021) as here shown in Our World in Data.

That 3rd injection is the one after which the IgG4 paper authors saw the most difference in IgG3/IgG4 ratios, but not necessarily the greatest increase in cases of cancer.
Let’s consider the whole immune system, not only immunoglobulins, as necessary to protect against the ravages of cancer. Immune cells and cytokines, and their exquisitely coordinated and synergistic functions, must be protected from the destructive events initiated by irreversible experimental injections of novel products, such as the mRNA vaccines.